BACKGROUND
COVID-19 is a serious disease that has rapidly spread around the world, posing a significant threat to human health and life. In addition to its medical and societal effects, the COVID-19 pandemic has led to increased psychological distress, such as anxiety and depression (Dong et al., 2021). In our study, we use the term ‘fear’, rather than the more common term ‘anxiety’, to describe peoples’ feelings about COVID-19 infection and COVID-19 vaccination. As defined in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), published by the American Psychiatric Association (2013), ‘Fear is the emotional response to real or perceived imminent threat, whereas anxiety is anticipation of future threat’ (p. 189). Fear therefore applies to both real infection and vaccination (fear of side effects or fear of injection).
Many studies have indicated that fear of COVID-19 infection has broad demographic, economic, social and psychological determinants. For example, psychological factors include intolerance of uncertainty and general risk aversion (Millroth & Frey, 2021), anxiety about one’s health and the health of family members (Oniszczenko, 2021), regular use of media and social media (Pimenta et al., 2020) and limited knowledge about COVID-19 (Cerda & García, 2022). The factors that have determined the level of emotional distress in individuals during the pandemic include experiencing stress, anger and fear (Kabasawa et al., 2021), health anxiety (Nürnberger et al., 2022) and, for professionals directly involved in patient care, the risk of contact with infected patients and the experience of quarantine (Sirosis & Owens, 2021).
However, little is known about the role of personality traits in individuals’ fear of COVID-19 infection. Some studies have examined the importance of the personality traits included in the Big Five model in relation to COVID-19. For example, Aschwanden et al. (2021) have found a relationship between the traits of neuroticism, extraversion, and conscientiousness and pandemic behaviour, such as expressing anxiety or undertaking preparations (see also Kohút et al., 2021). Zacher and Rudolph (2021) found that emotional stability was associated with a low level of perceived COVID-19 stressfulness, while extraversion was associated with a high level of perceived stressfulness. Fernández et al. (2020) reported that neuroticism significantly influenced the level of distress experienced by women in quarantine conditions. An association between neuroticism and overall pandemic anxiety was also established by Kumar and Tankha (2022). Moreover, Ikizer et al. (2022) suggested that neuroticism may be a good predictor for stress associated with the pandemic. However, the analysis by Fink et al. (2021) indicated that personality traits, including neuroticism, have only a small effect on behaviour related to the COVID-19 pandemic.
Several studies have shown that personality traits can contribute to attitudes about COVID-19 vaccination. For example, a study by Yanto et al. (2021) revealed that vaccination readiness may be related to higher levels of agreeableness and neuroticism. Similarly, Lin and Wang (2020) observed a relationship between high levels of agreeableness, conscientiousness and emotional stability and favourable attitudes towards COVID-19 vaccination (see also Salerno et al., 2021).
Many researchers have indicated that unwillingness to vaccinate against COVID-19 may be due to an individual’s level of fear of COVID-19 infection. Low or no fear of COVID-19 infection is associated with rejection of vaccination (Sekizawa et al., 2022). Similarly, Scrima et al. (2022) found that fear of COVID-19 infection reduces the reluctance to vaccinate; however, fear aroused by COVID-19 conspiracy theories and inadequate knowledge of the disease prevents vaccination. Bendau et al. (2021) reported that fear of COVID-19 infection promotes acceptance of vaccination, but at the same time fear of the social and economic aftermath of the pandemic weakens vaccination readiness. According to Mertens et al. (2022), while fear of COVID-19 infection increases vaccine readiness, the perceived risk of vaccination reduces vaccine readiness. On the other hand, Lee and You (2022) suggested that acceptance of vaccination may be due to perceived susceptibility to infection as well as the perceived benefits of vaccination.
STUDY OBJECTIVES
The primary objective of our correlational, cross-sectional study was to determine the relationship between fear of COVID-19 infection and fear of vaccination against COVID-19. We also wanted to investigate the role of the personality traits postulated by the Big Five model in this relationship. Given the functional importance of the Big Five personality traits, we expected that both fear of COVID-19 infection and fear of COVID-19 vaccination would be negatively correlated with emotional stability. We also assumed that fear of infection would mediate the relationship between emotional stability and fear of COVID-19 vaccination. Furthermore, we postulated that a high level of extraversion, openness to experience, and conscientiousness would be associated with a low level of fear of vaccination.
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
The study sample consisted of 462 participants aged 18 to 75, with a mean age of 32.22 years (SD = 12.58). Participants were recruited from the general population and included 286 women and 176 men. Detailed characteristics of the entire study sample are presented in Table 1.
Table 1
Sociodemographic variables in the studied sample (N = 462)
The study participants were divided into two groups for the statistical analysis. The first group included people with a previous COVID infection, and the second group included people without a previous COVID-19 infection. It should be recalled that the population from which the study participants were recruited consisted of two different groups: people who had previously been infected with COVID-19, and people who had not had such an experience.
PROCEDURE
All data were collected using an online recruitment platform between November 2021 and February 2022, that is, during the fourth wave and the beginning of the fifth wave of the COVID-19 pandemic in Poland. Participation in the study was anonymous and fully voluntary. Participants were not remunerated for their participation. All participants received information about the purpose of the study, the confidentiality of collected data, and the possibility of withdrawing from the study at any time without giving a reason. The research procedure strictly followed ethical principles for human research and was approved by the Research Ethics Committee at the Faculty of Psychology at the University of Warsaw (ref: 16-11-2020).
MEASURES
The Big Five personality traits. The Polish version of the Ten-Item Personality Inventory (TIPI; Gosling et al., 2003; Sorokowska et al., 2014) was used to assess the Big Five personality traits. Cronbach’s α coefficients for the current study were as follows: emotional stability (.73), extraversion (.75), openness to experience (.44), agreeableness (.63) and conscientiousness (.72).
COVID-19-related fear. An 11-point numerical rating scale was used to measure the intensity of participants’ fear of the COVID-19 infection as well as their fear of vaccination against COVID-19 (Fitzpatrick et al., 2020; Sigorski et al., 2020). Participants rated the severity of their fears on a scale from 0 (I feel absolutely no fear) to 10 (I feel unimaginable fear).
STATISTICAL ANALYSIS
All computations were performed using IBM SPSS Statistics (Version 27). The relationships among variables were examined with Pearson product-moment coefficients. The differences between COVID-19 groups with diagnosed prior infection and no diagnosed prior infection were computed using independent two-sample t-tests. Predictions of fear of vaccination against COVID-19 based on the previous COVID-19 infection, the fear of COVID-19 infection and Big Five personality traits were estimated using multivariate linear regression analysis in the entire sample. The mediation analyses were conducted via the PROCESS macro for SPSS (Version 3.5), Model 4 (Hayes, 2018). A bootstrapping procedure with 5,000 sample draws and bias-corrected standard errors was used to estimate the direct and indirect effects (Preacher & Hayes, 2008).
RESULTS
Table 2 presents the Pearson r correlation coefficients among COVID-19-related fear, fear of COVID-19 vaccination, the Big Five personality traits, and age.
Table 2
Pearson r correlations for the study variables (N = 462)
As shown in Table 2, almost all correlation coefficients are small to medium. Positive correlations with COVID-19-related fear were found for fear of COVID-19 vaccination and age, while negative correlations were found for emotional stability, openness to experience, and agreeableness. Fear of COVID-19 vaccination correlated negatively with emotional stability and openness to experience. Means, standard deviations, and t-test statistics for the study variables in the diagnosed and undiagnosed COVID-19 groups are displayed in Table 3.
Table 3
Means, standard deviations, and t-test statistics for the study variables in the group of individuals with previous COVID-19 infection (N = 198) and the group of individuals without previous COVID-19 infection (N = 264)
According to the t-test values, there were statistically significant differences between the groups regarding fear of COVID-19 vaccines and emotional stability. For participants who had previously been infected with COVID-19, the fear of COVID-19 vaccines was significantly higher than for participants who had not been infected with COVID-19. Those diagnosed with COVID-19 were also less emotionally stable compared with undiagnosed individuals and were less open to experience (not significant).
To determine the extent to which previous COVID-19 infection, COVID-19-related fear and the Big Five personality traits can be viewed as predictors of fear of COVID-19 vaccination, we performed a multivariate linear regression analysis. Based on the regression coefficients, previous COVID-19 infection (β = –.15, p < .001), COVID-19-related fear (β = –.13, p = .004) and emotional stability (β = –.17, p = .002) were found to be significant predictors of fear of COVID-19 vaccination (adjusted R2 = .06). The results are summarized in Table 4.
Table 4
Multivariate linear regression analysis of previous COVID-19 infection, COVID-19-related fear and the Big Five traits as predictors of fear of vaccine against COVID-19 in the whole sample (N = 462) with variance inflation factor (VIF)
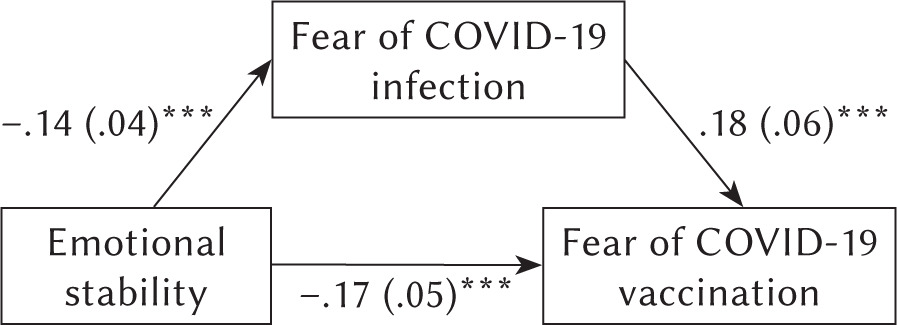
We conducted an analysis using a bootstrapping procedure, with fear of COVID-19 as the mediator between emotional stability and fear of COVID-19 vaccination in the studied group. The analysis showed a significant indirect effect of emotional stability on fear of COVID-19 vaccination through the mediator of fear of COVID-19 (effect = –.02, SE = .01, 95% CI [–.05, –.01]). The individual pathways in the mediation analysis are displayed in Figure 1.
DISCUSSION
The results of our study showed a positive correlation between fear of infection and fear of COVID-19 vaccination. Both fears were negatively correlated with emotional stability and openness to experience, while agreeableness was negatively correlated only with fear of COVID infection. A comparison of individuals with a previously diagnosed COVID infection and those without a previously diagnosed infection showed that those with a prior COVID infection have a higher level of fear of vaccination, are less emotionally stable and less open to experience (not significant). Among personality traits, emotional stability was the best predictor of fear of COVID vaccination and probably fear of COVID infection may serve as a mediator in the relationship between emotional stability and fear of vaccination.
We found that fear of COVID-19 infection was positively correlated with fear of COVID-19 vaccination. Yeşiltepe et al. (2021) reported a similar result, finding a positive correlation between fear of COVID-19 and COVID-19 vaccine hesitancy. The reasons for hesitancy were concerns about the side effects of vaccination in the absence of evidence about its effectiveness and reliability. The results of some studies indicate that the fear of vaccination against COVID-19 may be associated not only with anticipated short-term side effects of vaccination, such as allergic reactions, but also with long-term effects such as autoimmune and neurological reactions (Holzmann-Littig et al., 2022; see also Tahir et al., 2021).
Our result contrasted with Sekizawa et al. (2022), who reported that a low level of fear of COVID-19 in individuals was associated with unwillingness or indecision regarding being vaccinated against COVID-19. In our study, as demonstrated in Table 3, participants with a prior COVID-19 infection had a significantly higher level of fear of vaccination compared with participants without a prior COVID-19 infection, suggesting that previously infected individuals are less motivated to accept the vaccine than their never-infected counterparts. Some researchers have suggested that fear of vaccination may arise among hesitant people because of their anxiety and depression as well as concerns about vaccine efficacy, including vaccines in general and vaccine side effects (Nguyen et al., 2022). Scrima et al. (2022) showed that fear of COVID-19 infection reduces hesitancy and reluctance to vaccinate; however, the fear aroused by COVID-19 conspiracy theories and inadequate knowledge of the disease prevents vaccination. Yang et al. (2021) noted that only conspiracy theories about the vaccines themselves, not COVID-19 in general, were relevant to the decision to abstain from vaccination. Our findings suggest that individuals who have already had a COVID-19 infection are likely to develop beliefs about their lack of control over the epidemic and about vaccine ineffectiveness (see also Malesza & Kaczmarek, 2021). Peoples’ awareness of the limited COVID-19 treatment options, belief in conspiracy theories and moderate confidence in government communications that encourage vaccination and emphasise the safety of COVID-19 vaccines may also be significant here (see also Paul et al., 2021). It is noteworthy that Freeman et al. (2021) described a less-known risk factor for COVID-19 vaccine hesitancy: blood-injection-injury phobia, which could explain approximately 10% of COVID-19 vaccine hesitancy cases.
We believe that the positive correlation between fear of infection and fear of vaccination may be due to two slightly different mechanisms, namely ‘emotional’ and ‘cognitive’. Fear of becoming infected with COVID-19 comes from knowing the dangers of contracting the SARS-CoV-2 virus or its mutations, up to and including death. However, even if a significant proportion of the population judges that the risk of contamination is relatively low, those with conspiratorial thinking (e.g., the refusal to participate in a ‘large genetic experiment’ based on mRNA technology), low trust in social institutions and certain religious beliefs will favour vaccine rejection (Stamm et al., 2022). Some authors have pointed to the excess of misinformation on the Internet, especially regarding the misrepresentation of vaccine side effects, as causing fear of vaccination (Fieselmann et al., 2022; see also Ganie & Mukhter, 2022). According to Zhou et al. (2022), fear of COVID-19 may be an important mediating factor between the negative media influence on attitudes towards vaccination and COVID-19 vaccine hesitancy.
We theorise that the Big Five personality traits may be significant factors contributing to the increase in fear about the vaccine. As correlative data showed (see Table 2), fear of COVID-19 infection and fear of vaccination negatively correlated with emotional stability and openness to experience. We found that participants previously infected with COVID-19 were less emotionally stable than those with no prior infection.
The relationship between neuroticism and the level of fear of COVID-19 infection and fear of vaccination is well known (Fernández et al., 2020; Ikizer et al., 2022; Kumar & Tankha, 2022; Troisi et al., 2021; Zacher & Rudolph, 2021). Our research showed that people previously diagnosed with COVID-19 have significantly higher levels of neuroticism (i.e., they are less emotionally stable) compared to people without a prior COVID-19 diagnosis. While statistically significant, the difference between the two groups is small, and it is possible that this result is due to the TIPI construction used in our study and discussed by some researchers (DeBell et al., 2022). Nevertheless, individuals diagnosed with COVID-19 may experience severe stress and initiate ineffective ways of coping with stress, exacerbated by inadequate social support and social isolation, during the disease. This situation causes an increase in the level of neuroticism, analogous to some survivors of natural disasters who experience an increase in another personality (temperament) trait, such as emotional reactivity, that is, the tendency to respond intensely to stressful stimuli (Zawadzki et al., 2009).
Neuroticism, as a personality trait, can increase the degree to which fear becomes generalized (Garcia & Zoellner, 2017). In our study, the fear of COVID-19 infection could be generalized to fear of vaccination due to neuroticism.
Openness to experience was the second feature of the Big Five model that we found to be weakly related to the fear of COVID-19 infection and vaccination against COVID. The relationship between openness to experience and the COVID-19 pandemic is ambiguous. Nikčević et al. (2021) found a link between the traits of neuroticism and openness to experience and COVID-19-related anxiety and COVID-19-related anxiety syndrome. The results of the Proto and Zhang (2021) study suggested that a high level of both openness to experience and extraversion contributed to the deterioration of mental health during the COVID-19 pandemic, whereas Mo et al. (2021) reported that a high level of openness to experience was positively associated with a high willingness to be vaccinated against COVID-19. The results of our multivariate linear regression analysis demonstrated that both COVID-19-related fear and emotional stability were predictors of fear of being vaccinated against COVID-19. Together, both COVID-19 fear and emotional stability accounted for approximately 4% of the variance in fear of COVID-19 vaccination. Although personality traits may be associated with perception of situations, in the case of the COVID-19 threat, personality may have less influence on human behaviour compared to other factors, such as when individuals believe conspiracy theories and perceive the pandemic as a deception (Hettich et al., 2022).
The mediation analysis showed that emotional stability may directly and indirectly influence the fear of COVID-19 vaccination. The relationship between emotional stability and fear of vaccination is likely mediated by fear of COVID-19 infection.
As Barlow et al. (2014) indicated, fear is one of the negative emotions that is considered an integral part of neuroticism. In an experimental study, Kumari et al. (2007) described a positive correlation between neuroticism and the fear of shock. Additionally, Reynaud et al. (2012), in a study based on psychophysiological research, suggested that fear may be influenced by neuroticism. Thus, it is possible that fear and neuroticism, being related to each other, can serve as both independent variables and as mediators.
Our results from the mediation analysis were based on a one-time correlation study and therefore should be interpreted with caution, as the findings may reflect mediating or confounding factors (MacKinnon et al., 2000). We believe that these results require verification in future research.
LIMITATIONS
Our study has some limitations. We did not control for disease severity, when the COVID-19 infection was diagnosed, duration of disease or when it ended and whether it was a one-time or a repeated infection. We also did not collect data on comorbidities that could have impacted the fear of infection and fear of vaccination. We did not control for factors other than the fear of infection that could influence the fear of vaccination, such as having children or infections among loved ones. Given this context, we recommend a future study using mixed quantitative and qualitative methods to better elucidate the relationships being analysed.
Despite our relatively large sample, its representativeness may be limited, as it included primarily women and younger people (those aged 60 years or over accounted for 4.54% of the entire sample). Potential older participants may not have been connected to the Internet or may have had limited access. Our study was based on a cross-sectional design, which significantly limited the possibility of determining causal relationships between the studied variables. The results of our study’s mediation analysis also require further verification.
CONCLUSIONS
In this study, we found a positive link between fear of COVID-19 infection and fear of the COVID vaccine. Both types of fear were also negatively correlated with emotional stability and openness to experience. People diagnosed with COVID-19 had significantly higher levels of fear of the vaccine and lower levels of emotional stability compared to those who had not been infected. COVID-19-related fear and emotional stability were good predictors of fear of the COVID vaccine, and fear of COVID-19 infection likely serves as a mediator between emotional stability and fear of vaccination against COVID-19. This relationship should be further examined in future studies.