BACKGROUND
SECONDARY TRAUMATIC STRESS
Police officers, as part of their professional life, are exposed to various types of stressful situations. Conn and Butterfield (2013) distinguish three categories of stressful situations in this group: organizational stress, police stress-critical incidents, and secondary exposure to trauma, which leads to secondary traumatic stress. Organizational stressors comprise personnel issues and workplace difficulties in the form of paperwork or shiftwork. Critical stress situations concern incidents in which the safety of police officers is threatened; such events are connected with the risk of posttraumatic stress disorder (PTSD) development. Finally, exposure to traumatic events experienced by other people, most commonly accidents, assaults or violent episodes, and the suffering of others can also lead to secondary traumatic stress. This final group of stressors is a very important one, as policemen, like doctors, nurses, psychologists, and social workers, are considered as helping professionals. These professionals are seen as having to bear a high emotional burden while working with people after experiencing traumatic situations (Maran et al., 2020); despite this, relatively little research has been devoted to development of secondary traumatic stress as a result of secondary trauma exposure.
Secondary traumatic stress (STS) is described as the emotional and behavioural consequences experienced by person after gaining knowledge about the individual’s stressful situation (Figley, 1995, 2002). Figley regards STS as a natural consequence of behaviour and emotion stemming from the information about traumatic situations experienced by others, and “the cost of caring” for them.
According to Baird and Kracen (2006), STS is a group of psychological symptoms that resemble those of PTSD, but unlike PTSD, it arises from contact with people who are experiencing the effects of trauma. In this sense, the symptoms of secondary traumatic stress may be similar to those of posttraumatic stress disorder, which are observed in individuals who directly experience traumatic events. According to the DSM-5, the symptoms can be classified according to the following four criteria: avoidance, intrusion, and alterations in arousal or reactivity and negative alterations in cognitions or mood (APA, 2013).
The phenomenon of STS has also been referred to as compassion fatigue, which preceded the term STS (Figley, 1995), vicarious traumatization, which describes changes in the worldview of helpers occurring as the effect of empathic involvement with people who experience trauma (McCann & Pearlman, 1990), or burnout, used to describe the emotional exhaustion, depersonalization and loss of self-efficacy as a result of lengthened work (Bakker & Hueven, 2006).
It is worth noting that STS can result in various consequences, including disruptions in the personal and professional identity of workers, the manifestation of maladaptive coping strategies, and negative feelings, anxiety, depression, sleep disorders and reducing resilience (Maran et al., 2020). It may also decrease the effectiveness of the work performed, reduce work satisfaction and worsen the quality of life of professionals working with trauma victims (Ogińska-Bulik & Juczyński, 2020).
STS AMONG POLICE OFFICERS
There has been little research into the prevalence of STS among police officers and the few studies performed have produced heterogeneous results. Data provided by Molnar et al. (2017) show that representatives of the emergency services, including police officers, experience fewer negative consequences of secondary trauma exposure than other professional groups. This is confirmed by a recent meta-analysis of 31 studies conducted among firefighters, policemen and rescue and search personnel (Greinacher et al., 2019), which showed that STS occurred in 4-13% of respondents. Similarly, a study by Hargrave (2010) in New Zealand found that only 3.5% of police officers revealed significant symptoms of STS.
However, Maran et al. (2020) found that police officers experience STS at a higher rate than health care workers. High intensities of STS symptoms have also been observed in the representatives of emergency services helping children who have suffered trauma, particularly policemen. The majority of police detectives from the South African Police Service who worked in the Family Violence, Sexual Offences and Child Protection unit (Cronje & Vilakazi, 2020) reported some degree of STS symptoms, which the authors attribute to frequent exposure to traumatised complainants. Research conducted in Wales and England among police officers from the Child Abuse Investigation Unit indicated that increased exposure to childhood sexual abuse was connected with a higher degree of STS (Hurrell et al., 2018). Surveys of police officers employed in family protection units (MacEachern et al., 2019) found that 40% of respondents demonstrated a moderate severity of STS, and 11% high or very high. The symptoms of intrusion were particularly intense. Other studies of police officers involved in investigating child abuse online revealed that 70% of respondents show symptoms of STS, and 25% of them to a high degree (Bourke & Craun, 2014).
THE RELATIONSHIP BETWEEN PERSONALITY, RUMINATIONS AND STS
Many factors may induce the development of STS symptoms, some of which are linked to the work environment, containing workload, social support received from supervisors and co-workers, or work satisfaction, with a further role being played by individual characteristics including personality and cognitive trauma processing skills (Ogińska-Bulik & Juczyński, 2020; Ogińska-Bulik et al., 2021). Two of the personality traits believed to play a particularly important role in the development of STS symptoms are neuroticism and introversion.
Neuroticism and introversion have been found to foster negative thinking, which favours the development of PTSD. Neurotics, as introverts, are more pessimistic and less likely to seek social support (Tehrani, 2010). Therefore, similar dependencies can be expected with regard to STS. A positive relationship between neuroticism, introversion and STS has been demonstrated in studies conducted among investigators dealing with the problem of online child abuse (Tehrani, 2016). A study of medical personnel in Romania found neuroticism, extraversion and conscientiousness to be predictors of dysfunctional beliefs, treated as an indicator of secondary traumatization; these beliefs were associated positively with neuroticism, and negatively with conscientiousness and extraversion (Măirean & Turliuc, 2013). In turn, studies conducted among cemetery workers (Colombo et al., 2019) showed STS to have positive relationships with negative affect, associated with neuroticism, and negative relationships with positive affect, characteristic of extraversion. In addition, in a study of a group of nurses and physicians exposed to secondary trauma, a low level of STS symptoms was found to be connected with a higher degree of perceived positive posttraumatic changes among individuals who revealed a great level of conscientiousness, agreeability and openness to new experience (Măirean, 2016).
Another factor that may influence the severity of STS in helping trauma victims is ruminating about the event experienced by the client. Such rumination pertains to repeated and recurrent thinking about an experienced situation and its outcomes (Michael et al., 2007). It may also be considered as dysfunctional way of regulating emotions and coping with stress (Nolen-Hoeksema et al., 2008). Ehlers and Clark (2000) stress that in the face of a traumatic event, activity both cognitive and emotional may be one of the most crucial variables influencing the effects of experienced situations, including the development of PTSD symptoms. According to the cognitive model of PTSD (Ehlers & Clark, 2000) after perceiving a traumatic situation as a danger, individuals usually try to deal with it by rumination, a maladaptive way of cognitive processing which favours the development of PTSD symptoms.
Nevertheless, it must be pointed out that prior research on the issues of trauma consequences (Calhoun et al., 2010; Cann et al., 2011) differentiate between two forms of trauma-related ruminations. The first, intrusive ruminations, are mechanical, disastrous, uncontrolled and undesirable thoughts unconnected with solving the problem. The second, deliberate ruminations, consist of more controlled and productive thoughts focused on trying to solve the problem and understand an adverse situation. Research from this field has proved a positive relationship of especially intrusive ruminations with development of posttraumatic stress disorder symptoms (Cann et al., 2011; Ehlers & Clark, 2000; Ehring & Ehlers, 2014; Ogińska-Bulik, 2018). Therefore, a similar relationship can be expected with regard to STS.
Ruminations were found to positively correlate with intrusion in a group of medical staff in Romania (Turliuc et al., 2015). In addition, positive associations were found between STS symptoms and intrusive as well as deliberate ruminations in a group of probation officers working with trauma victims (Ogińska-Bulik & Juczyński, 2020). Ruminations are also related to personality traits, and most of all with neuroticism (Roelofs et al., 2008; Zanon et al., 2016). Intrusive ruminations about an experienced event have been found to be positively connected with neuroticism and negatively with openness to experiences in people struggling with cancer (Ogińska-Bulik, 2017).
In addition, ruminations may directly influence the negative consequences of trauma, and may mediate the associations between personality traits and certain negative aspects of health, including STS symptoms. Research conducted among students (Roelofs et al., 2008) showed that rumination plays a role as a mediator in the relationship of neuroticism with depression and anxiety symptoms occurrence. Data obtained by Turliuc et al. (2015) confirmed that rumination and suppression mediated the effects of dysfunctional beliefs about oneself and about the world on intrusion in a group of medical staff. Ehring and Ehlers (2014) found that intrusive ruminations play a role as mediators in the relationship between emotion regulation difficulties and symptoms of posttraumatic stress disorder in road accident victims. The same results have been obtained in studies conducted among cancer patients (Ogińska-Bulik & Michalska, 2019). No studies have yet reported a relationship between personality, rumination and STS among police officers, including the role of ruminations as mediators.
The purpose of the present study was to establish the prevalence of STS symptoms among police officers after secondary trauma exposure, and to determine its relationship with personality traits and ruminations. The research also examines the mediating role of ruminations in the associations between personality and secondary traumatic stress. To achieve this, the following research questions were addressed:
What is the severity of secondary traumatic stress symptoms in the group of police officers exposed to secondary trauma?
Are personality traits and ruminations related to the severity of STS symptoms?
Do ruminations play the role of mediators in the relationship between personality traits and secondary traumatic stress?
Based on the Ehlers and Clark (2000) PTSD model, it may be supposed that both personality, especially neuroticism, and ruminations, particularly intrusive ones, will be associated with STS symptoms, and that ruminations about the situations will play a mediating role in the relationship between personality and STS.
PARTICIPANTS AND PROCEDURE
PARTICIPANTS
The research took place in the period from June to August 2021 at the Police Academy in Szczytno (Poland). The project was specifically approved by the Police Headquarters. The study involved 296 police officers, all of whom were university graduates who had continued in postgraduate vocational training. These officers work on a daily basis in police organizational units throughout Poland. The study was voluntary and anonymous. As 61 policemen did not deal with trauma victims in their work, the data were collected from a total of 235 police officers (79.4% of the sample) who worked directly with trauma victims. Their clients have experienced various types of traumatic events. The most common events were various types of violence (n = 129), accidents (n = 60), and death (n = 78). The participants represented three divisions of the police force: Prevention (n = 59; 25.1%), Criminal (n = 149; 63.4%) and Supportive (n = 27; 11.5%). The group comprised 178 men (75.7%) and 57 women (24.3%).
The age of the individuals ranged from 30 to 60 years (M = 40.79, SD = 3.96) and the length of service as a police officer was from 5 to 30 years (M = 15.41, SD = 3.74); in addition, the length of time working as a police officer assisting trauma victims ranged from 3 to 26 years (M = 12.81, SD = 4.62). The weekly number of hours at work that was spent helping trauma victims varied from 1 to 40 (M = 9.91, SD = 9.82), and the time devoted to providing direct help to clients ranged from 1% to 100% (M = 20.63, SD = 20.71), expressed as a proportion of the total work time. In the study group, the majority of examined police officers (65.9%) had experienced traumatic events directly. The most commonly experienced traumatic events included accidents (n = 48), life-threatening disease (n = 33), violence (n = 22) and the death of a loved one (n = 21).
MEASURES
The survey comprising questions about gender, age, own history of trauma, work experience, the weekly number of hours devoted to work with trauma victims, and time devoted to providing direct help to them, expressed as the proportion of total work time, was used in the study. The last three variables were taken as an index of exposure to secondary trauma. In addition, the following three standard research tools were used:
Secondary Traumatic Stress Inventory (STSI) is a modified adaptation of the Post-Traumatic Stress Disorder Checklist developed by Weathers et al. (2013) in the Polish adaptation by Ogińska-Bulik et al. (2018). It is a self-report measure created for the purpose of monitoring, screening, and diagnosing individuals providing help to trauma survivors. It contains 20 items/reactions to traumatic situations (“Repeated, disturbing, and unwanted memories of the stressful experience”), which refer to symptoms of posttraumatic stress disorder, that is negative alterations in cognitions and mood, avoidance, intrusions and alterations in arousal and reactivity. In line with the instruction, recipients provide answers on a 5-point scale from 0 (not at all) to 4 (extremely) to indicate to what level each symptom bothered them over the last month in connection with the help they provided. Cronbach’s α coefficient for the Polish adaptation of PCL-5 is .90, and for individual factors, it assumes the following values .71, .85, .89, .87 (Ogińska-Bulik & Juczyński, 2020).
The NEO Five-Factor Inventory (NEO-FFI), created by Costa and McRae (1989), in the Polish adaptation by Zawadzki et al. (1998) was used to assess five personality dimensions: extraversion, neuroticism, openness to experience, conscientiousness and agreeableness. It consists of 60 items (“I am not a worrier”) scored on a scale from 1 (decidedly disagree) to 5 (completely agree). The Cronbach’s α coefficient for the Polish adaptation ranges from .60 to .82.
The Event Related Rumination Inventory (ERRI) was created by Cann et al. (2011) and adapted to Polish conditions by Ogińska-Bulik and Juczyński (2015). It contains two subscales; each subscale consists of 10 statements. The first one (“I thought about the event when I did not mean to”) concerns intrusive ruminations, and the second (“I thought about whether I could find meaning from my experience”) concerns deliberate (reflective) ones. The individuals answer each statement on a 4-point Likert scale from 0 (not at all) to 3 (often). The scores are calculated independently for each subscale. Cronbach’s α coefficient for the Polish version is .96 for intrusive ruminations and .92 for deliberate ruminations.
STATISTICAL ANALYSES
IBM SPSS software, version 25, was used for statistical analysis. As the obtained data either met or approximated the criteria of normality, parametric tests were employed (Student’s t-test, F test analysis of variance and Pearson’s correlation coefficients). The means for the analysed variables and the correlation coefficients were calculated (Table 1). The PROCESS procedure by Preacher and Hayes (2008) was used to establish the role of ruminations as mediators in the relationship between personality traits and secondary traumatic stress. Personality dimensions acted as predictors, STS played the role of the dependent variable, and both deliberate and intrusive ruminations about situations played the role of mediators. The effect of mediation exists when the mediator decreases the predictive value of the independent variable for the dependent variable.
Table 1
Descriptive statistics and correlation coefficients of analysed variables (N = 235)
RESULTS
The mean STS score was lower than that obtained from a previous study of professionals working with trauma survivors (M = 24.14, SD = 16.11; Ogińska-Bulik & Juczyński, 2020). Assuming a cut-off point for STSI of 33 points, 211 police officers (89.8%) reported a low level of STS, while only 24 of them (10.2%) reported a high level.
The severity of secondary traumatic stress symptoms was not affected by gender (men: M = 14.09, SD = 12.63; women: M = 13.24, SD = 12.80, t = 0.65) nor the police division (Prevention: M = 13.71, SD = 10.27; Criminal: M = 14.42, SD = 13.24; Supportive: M = 11.33, SD = 14.06, F = 0.69). STS symptoms were not found to be significantly associated with age (r = .02), total work experience in the police force (r = .09) or weekly number of hours devoted to work with trauma victims (r = .11). Weak relationships were observed between STS symptoms and work experience as a police officer working with trauma victims (r = .18, p = .008) and time devoted to providing direct help to them, expressed as a proportion of the total work time (r = .18, p = .018. A previous history of trauma differentiated the severity of STS symptoms among police officers: those who experienced traumatic events themselves revealed a higher severity of STS (M = 15.36, SD = 13.84) compared to those who did not (M = 11.02, SD = 10.60).
Based on the criteria developed for a Polish population, expressed as sten scores, the police officers participating in the study demonstrated a rather low level of neuroticism, a rather high level of extraversion, and an average level of conscientiousness, agreeableness and openness to experience (Zawadzki et al., 1998). According to the criteria of the Polish version of the ERRI (Ogińska-Bulik & Juczyński, 2015) they also reveal a low level of both forms of rumination.
It was found that symptoms of secondary traumatic stress are positively related to both types of ruminations, with a stronger relationship with intrusive ruminations. In addition, STS symptoms appeared to have a stronger relationship with neuroticism (positive) and a weaker one (negative) with conscientiousness, agreeableness and openness to experience. In general, the STS symptoms demonstrated much weaker correlation coefficients with personality traits than with ruminations. Among the personality traits, only neuroticism positively correlated with ruminations; it also demonstrated a slightly stronger relationship with intrusive rumination than with deliberate rumination.
The identified links between personality, ruminations and STS symptoms make it possible to look for a more complex relationship, considering the role of ruminations as mediators. Only two models were significant (Figures 1 and 2) and they refer only to neuroticism.
Figure 1
Model of relations between personality trait in the form of neroticism, intrusive rumination and secondary traumatic stress.
Note. βab – indirect effect, βc – total effect, bc’ – direct effect, ***p < .001.
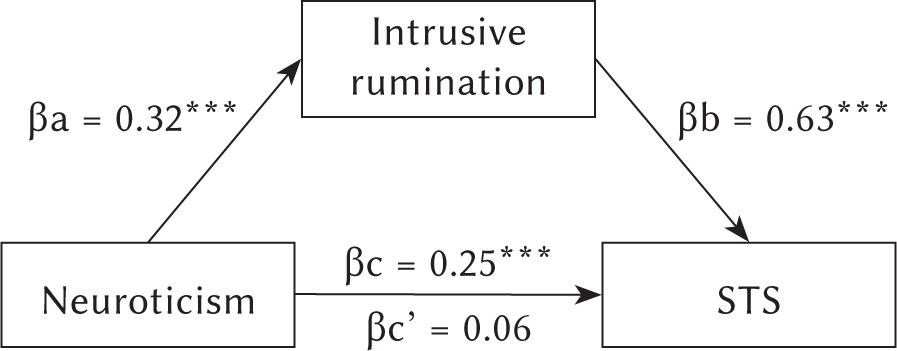
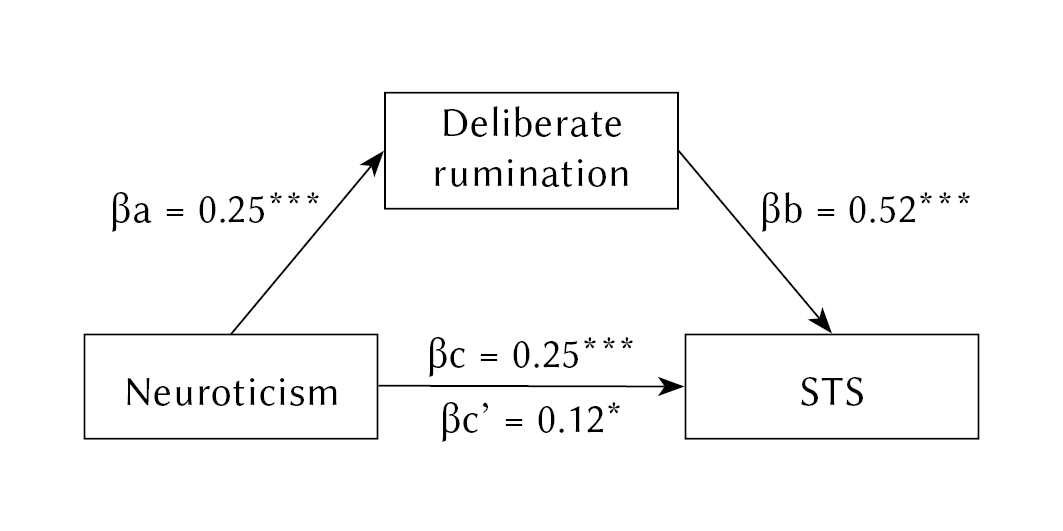
Figure 2
Model of relations between personality trait in the form of neroticism, deliberate rumination and secondary traumatic stress.
Note. βab – indirect effect, βc – total effect, bc’ – direct effect, *p < .05, ***p < .001.
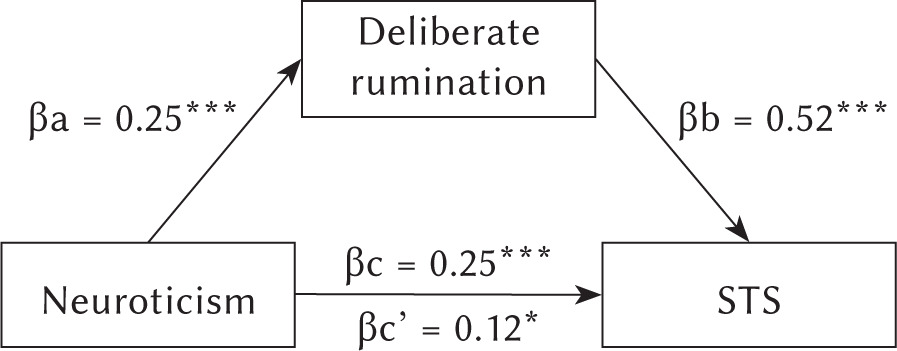
Neuroticism was found to be positively linked with intrusive ruminations (Figure 1). Both variables are positive predictors of STS, with ruminations being a much stronger predictor. The introduction of intrusive ruminations as a mediator in the association between neuroticism and secondary traumatic stress symptoms makes the relationship non-significant, which implies full mediation: the occurrence of STS symptoms is more closely associated with ruminative thinking than with neuroticism. In turn, the introduction of deliberate ruminations as a mediator in the relationship between neuroticism and STS symptoms (Figure 2) weakens the association between variables, which implies partial mediation: the relationship between neuroticism and STS is partially explained by deliberate rumination. Finally, the data from the mediation analysis indicate that it is not neuroticism, but rather ruminations, that have the greatest influence on increasing the likelihood of occurrence of STS symptoms.
DISCUSSION
Police officers working with trauma victims generally demonstrate a rather low intensity of secondary traumatic stress symptoms. The great majority of respondents (90%) present a low risk of secondary trauma stress disorder (STSD), and only 10% of police officers present a high probability of developing symptoms of STS. This is a much lower percentage than among paramedics (Ogińska-Bulik et al., 2021), social workers and probation officers (Ogińska-Bulik & Juczyński, 2020). This conclusion may suggest that police officers who work with victims of trauma have adequate ability to cope with the clients’ traumatic experience and are well prepared for practising their profession.
These data, indicating a rather low risk of STSD in Polish police officers, is largely consistent with results obtained in other countries (Greinacher et al., 2019; Hargrave, 2010; Maran et al., 2020; Molnar et al., 2017). They are also in line with previous research indicating a relatively low level of PTSD symptoms in policemen who were directly exposed to traumatic events, as confirmed by a meta-analysis of 28 studies collected from three continents (Asia, Europe and North America) indicating that the prevalence of PTSD among representatives of the emergency services does not exceed 10% (Berger et al., 2012).
Age, gender, police division, total length of service in the police force and weekly number of hours devoted to working directly with trauma victims were not associated with STS symptoms. However, experience as a police officer working with trauma victims and time devoted to providing direct help to them, expressed as a proportion of the total work time, did correlate with symptoms of STS, although weakly. In addition, police officers who themselves experienced traumatic events demonstrated a high intensity of negative symptoms of secondary exposure to trauma.
STS symptoms were more strongly associated with ruminations (especially intrusive) than with personality traits, among which neuroticism plays a key role. Both ruminations and neuroticism turned out to be positively correlated with STS. However, weak negative associations were observed between STS symptoms and conscientiousness, agreeableness and openness to experience. In addition, the police officers with a high level of neuroticism and who tend to intensively ruminate about the events experienced by the clients were found to be more prone to display the negative impacts of secondary trauma exposure. Our findings are partly consistent with data obtained by Tehrani (2016) showing a positive relationship between neuroticism, introversion and STS among investigators dealing with the problem of online child abuse. They are also consistent with data indicating positive associations between ruminations and symptoms of secondary traumatic stress obtained from other specialists who work with victims of trauma, such as medical personnel (Turliuc et al., 2015) or probation officers (Ogińska-Bulik & Juczyński, 2020).
The mediation analysis confirms that ruminations, especially the intrusive form, act as a mediator in the association between neuroticism and STS. A high tendency to rumination increases the likelihood of the occurrence of STS symptoms. As such, police officers who are not prone to ruminating about the traumatic events experienced by clients, even exhibiting a high level of neuroticism, are less likely to develop STS than those who are neurotic and show a strong tendency to ruminate.
The study results are consistent, at least partly, with data obtained by other studies, on the various negative effects of experienced stress (Ehring & Ehlers, 2014; Ogińska-Bulik & Michalska, 2019; Roelofs et al., 2008; Turliuc et al., 2015). Our findings confirm that certain methods of emotional regulation and coping with stress, mainly maladaptive ones, expressed as ruminations, may favour the development of the adverse effects of indirect trauma exposure. It indicates that the model created for posttraumatic stress disorder (Ehlers & Clark, 2000) can also be applied to STS.
The study does have some limitations. Its cross-sectional character does not allow for any inferences about causality. In addition, the group of participants was restricted to those receiving vocational training for university graduates. The group of participants was not characterized by homogeneity; most were men, and the group was dominated by police officers from the Criminal division, with the Supporting division being poorly represented. The association between STS symptoms in the police officers as well as the type of traumatic event experienced by the clients was not analysed, when in most cases it was multiple events. Further analyses did not address the history of trauma experienced by the officers, and as indicated, those who experienced traumatic events themselves showed a higher level of STS; indeed, it is possible that the relationship between STS and personality or ruminations would differ depending on whether the police officers themselves experienced the trauma or not. However, in this professional group it is difficult to clearly separate the occurrence of PTSD symptoms from STS.
The similarity between ruminations and one of the symptoms of STS, and also PTSD, i.e., intrusion, should be noted; nonetheless, these concepts are distinct. Ehring and Ehlers (2014, p. 1) stressed that “intrusive memories are sensory experiences of short duration that represent the experience of the trauma itself, whereas rumination is described as a train of thoughts of longer duration that elaborate on the experience”.
Despite the above-mentioned limitations, our findings contribute to the body of knowledge on the prevalence of the adverse results of exposure to secondary trauma in police officers, and on the association between personality and rumination. It is important to mention that the study employed a new tool, the Secondary Traumatic Stress Inventory, which was developed according to DSM-5 criteria.
The obtained results may inspire further studies; however, these should address other factors determining the negative consequences of secondary exposure to trauma, including many different indexes of cognitive processing of trauma such as disruption in core beliefs and other personality properties, e.g. self-efficacy or dispositional optimism. Moreover, a longitudinal approach would be desirable to capture the changes in the intensity of the adverse effects of secondary trauma exposure over time; it is important to consider the possibility of positive secondary posttraumatic change, revealed as secondary/vicarious posttraumatic growth.
This study has some practical implications, as it may be applied to devising prophylactic actions whose aim is to reduce the symptoms of STS. Such interventions should include expanding the competencies in coping with trauma, and should take into account both cognitive and behavioural remedial practices, including self-care. The importance of interventions directed against STS symptoms, and at promoting secondary posttraumatic growth, has been underlined by Molnar et al. (2017), and Ogińska-Bulik and Juczyński (2020). It is worth noting that self-care was a fairly popular and frequently described method of helping in a group of police officers (Conn & Butterfield, 2013).
CONCLUSIONS
Police officers working with trauma victims are prone to develop STS but its severity seems to be low. It was found that STS symptoms are significantly positively related to both types of ruminations, with a stronger relationship with intrusive ruminations. Neuroticism correlated more strongly with STS than other personality traits. Ruminations played the role of mediators in the relationship between neuroticism and STS. It may show the importance of this variable in the development of STS symptoms.