BACKGROUND
Parents create the first and most important relationship in a child’s life (Shaffer & Kipp, 2015), and thus the concept of parental sensitive responsiveness has garnered much attention among researchers in recent years (Bakermans-Kranenburg & van Ijzendoorn, 2018). A child’s relationship with their parents is based on them trusting their parents and knowing that the parents will take care of them and respond to their needs (van Ijzendoorn & Bakermans-Kranenburg, 2012). Thus, caregivers should be aware of and ready to perceive the child’s verbal and non-verbal cues and react to them appropriately (Ainsworth et al., 1974). Parental responsiveness can be displayed by initiating an interaction, changing the child’s position, providing an object of interest, cuddling, or showing sympathy to the child when they need it or if their needs cannot be completely fulfilled (e.g., when it would be dangerous to do so). Sensitive parents should be prompt in their responses, reacting in time to the cue, but also respect the dynamics of the child’s reactions. This caregiver-child relation requires that the parent’s reactions be flexible (Mesman et al., 2017). Parents with a high level of this construct can see things from their child’s point of view and focus on them and their needs (Mihelic et al., 2017). Moreover, a responsive parent tailors the child’s environment to their needs and gives them space and time to explore their environment (Belsky, 2014). Therefore, parental sensitive responsiveness to the infant’s cues is situationally dependent (Ainsworth et al., 1974) and depends on the child’s needs. Taking the above into consideration, this construct should be always analyzed contextually.
Parental responsiveness is beneficial for children, as it fosters development and social cognition (Hudson et al., 2015). Parental responsiveness is connected with better emotional understanding in children, more frequent displays of positive affect (Braungart-Rieker et al., 2014), and the development of secure attachment (Stern et al., 2015). Additionally, the responsiveness of parents is a predictor of children’s communication and early language development (Tamis-LeMonda et al., 2014).
Parental responsive reactions to infants’ cues are connected with the mother’s and father’s individual predispositions and characteristics. Empathy promotes parental responsiveness to a child’s needs (Belsky & Barends, 2002). Indeed, higher levels of empathy have been shown to be connected with higher sensitivity to stimuli that come from the child (Boorman et al., 2019). Dispositional empathy includes other-oriented perspective-taking (taking others’ point of view in social situations; Davis, 2004), which helps parents to respond adequately to a child’s cues (Stern et al., 2015), and empathic concern (compassion and care for others in need; Davis, 2004), which facilitates parental sensitive responses, monitoring of the child, and readiness to perceive new signals (Eisenberg & Eggum, 2009). The third aspect of empathy is personal distress (self-oriented feelings of personal anxiety and tension in interpersonal relations; Davis, 2004), which has been linked with greater frustration and anxiety in response to the child’s cues (e.g., crying; Barr et al., 2014; Kaźmierczak & Pawlicka, 2018).
Moreover, parental patterns of attachment in close relationships might affect their relationship with their child due to their sensitive responsiveness. Mothers and fathers who are avoidant and anxious in their close relationships display less responsive and sensitive parenting and show less support to their children (Jones et al., 2015). In general, research has indicated that the lower the attachment avoidance and anxiety, the higher the maternal sensitivity (van Ijzendoorn & Bakermans-Kranenburg, 2012).
The present study focused on the validation of the Parental Responsiveness Scale. Parental sensitive responsiveness to a child’s cues and/or needs is one of the dimensions of parents’ engagement with their children. Many behaviors are characterized by this type of responsiveness, but the following aspects are common to them all: they should be adequate, prompt, and provided with warmth and tenderness. This scale contains a description of different behaviors that match the definition of parental responsiveness (Ainsworth et al., 1974; Edwards et al., 2010). The aim of this study was to verify the one-dimensional structure of the proposed measure. To test convergent validity, positive correlations between parental sensitivity, empathic concern, and perspective-taking were expected and explored. Further, to test discriminant validity, negative correlations between personal distress and avoidance and anxiety in close relationships were examined.
Considering the above, the following hypotheses were formulated:
H1: The Parental Responsiveness Scale (PRS) will be a one-dimensional scale.
H2: Parental responsiveness will be higher when empathic concern and perspective-taking are higher and personal distress is lower.
H3: Parental responsiveness will be higher when anxious and avoidant attachment are lower.
PARTICIPANTS AND PROCEDURE
Two hundred and fifty parents of young children (including 186 mothers) took part in the study. Mothers were aged from 19 to 44 years (Mage = 28.92, SDage = 4.48) and fathers were aged from 22 to 42 years (Mage = 31.30, SDage = 4.10). 72.6% of mothers and 67.2% of fathers had completed third level education; 24.7% of mothers and 26.5% of fathers had completed high school; and 2.7% of mothers and 6.2% of fathers had vocational education. All participants were from Poland. The majority of parents had only one child (85.6%). The ages of the children of participating parents ranged from 1 to 18 months (Mage = 8.60, SDage = 4.06) and 50.8% were female.
Respondents were recruited via announcements on social media or activity groups for mothers. The sole inclusion criterion was having a child aged between 1 and 18 months. The set of questionnaires was provided via an online platform, to which the participants received a link. No personal data were gathered. Participation in the study was voluntary and there was no payment for participation.
MEASURES
Parental responsiveness. The Parental Responsiveness Scale (PRS; Anikiej & Kaźmierczak, 2019) was used. It consists of 13 items with a 7-point response scale from 1 (I strongly disagree) to 7 (I strongly agree). This scale contains different parental reactions to infant cues, for example: “I reciprocate my child’s smile”, “I name items that my child points at”, and “I make contact with my child when I see that they want it”. This tool has good reliability, with α = .90 in this study.
Empathy. Empathic Sensitivity Scale (Kaźmierczak et al., 2007). This questionnaire consists of 28 items; participants respond to these statements using a 5-point Likert response scale. Results are obtained for three subscales (components of dispositional empathy): 1) empathic concern – other-oriented emotional empathy (showing sympathy and concern to people in difficult situations; e.g., “I often have tender, concerned feelings for people less fortunate than me”); 2) perspective-taking – other-oriented cognitive empathy (taking other people’s points of view; e.g., “Sometimes I try to understand my friends better by imagining the situation from their point of view”); and 3) personal distress – self-oriented emotional empathy (the experience of negative emotions in response to others’ discomfort or suffering; e.g., “In difficult situations, I feel scared and lost”). All subscales are characterized by satisfactory reliability (values of α ranging from .71 to .78).
Attachment. Experience in Close Relationships-Revised – short version (Brennan et al., 1998; Polish adaptation by Lubiewska et al., 2016). This scale is composed of 16 items; participants assess attachment patterns in close relationships based on anxiety (e.g., “I am often worried that my intimate partner does not want to be with me”) and avoidance (e.g., “I prefer not to be too close to people who are important to me”) on a 7-point Likert scale from 1 (extremely untrue) to 7 (extremely true). The short scale displays better psychometric values than the full version (in Polish studies). In this study, it had good reliability for both anxiety and avoidance subscales (α = .89 and α = .86 respectively).
CONSTRUCTION OF THE TEST ITEMS AND THE RESPONSE SCALE
The first stage of the study consisted of the empirical identification of the factors of parental responsiveness towards children. First, a definition of parental responsiveness was prepared. In the next step, eight competent judges (psychologists with experience in developmental, family, or clinical psychology) were asked to give at least three examples of behaviors defined as responsive, based on the following definition:
Responsiveness is a kind of exchange between a parent and a child, serving to regulate emotions and behaviors. This is the physical and emotional availability of the parent and sensitivity to the child’s needs. It is a prompt response adequate to changing cues from the child. It involves monitoring, interpreting, and responding quickly and adequately to non-verbal and verbal signals from a child (Ainsworth, 1979; Ainsworth et al., 1974; Belsky & Barends, 2002; Leekers, 2010; Leerkes et al., 2009).
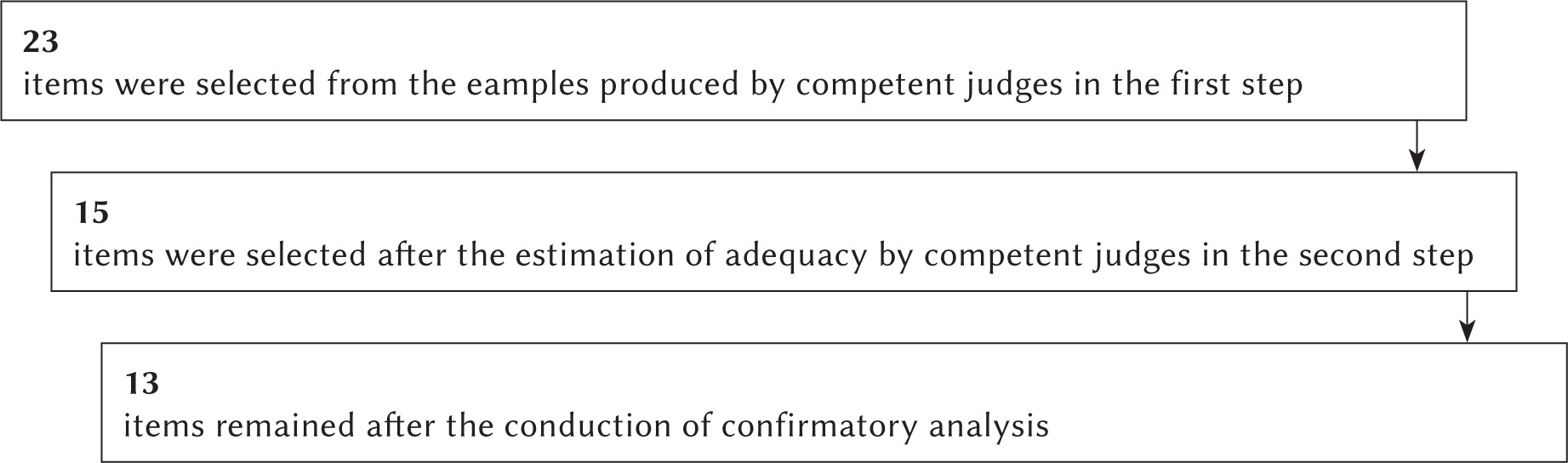
After a semantic analysis of the written answers, a set of 23 items was prepared. Then, ten different competent judges were asked to estimate the adequacy of each item to the definition, measured on a 7-point bipolar scale from –3 (It does not match the definition at all) to +3 (It fully meets the definition), with zero points treated as neutral.
After the assessment of the items by the independent psychologists, 15 items were selected as the most congruent with the definition.
STATISTICAL ANALYSES
Data analysis was performed using IBM SPSS 26.0 and MPLUS 7.2.
Factor analyses. Confirmatory factor analysis was carried out in MPLUS 7.2 using the WLSMV estimator (weighted least squares with adjusted means and variances) to verify the factorial structure of the PRS. As per recommendations, several fit indices were used in the analysis (Hu & Bentler, 1999): the comparative fit index CFI > .95, the Tucker-Lewis index (TLI; where values of .90-.95 are considered acceptable and values > .95 are considered good), and the RMSEA (where values ≤ .05 indicate good fit and values ≥ .10 indicate poor fit).
Correlational analyses. To estimate the relationships between the studied variables, Pearson’s r correlation coefficients were computed. The three aspects of empathy – empathic concern, perspective-taking, and personal distress – and two attachment styles – avoidance and anxiety in close relationships – were correlated with the results obtained on the PRS. These analyses were conducted using IBM SPSS 26.0.
RESULTS
STRUCTURE OF THE PARENTAL RESPONSIVENESS SCALE
Confirmatory factor analysis showed that the PRS had a one-factor structure. The standardized item loadings are shown in Table 1. The removal of the weakest item (3) and the strongest one (5; as it turned out to be redundant, given the definition of the scale) provided better fit indices. These results are shown in Table 2. The fit indices of this model and the overall fit of the model were satisfactory, χ2 = 184.07, df = 65, p < .001; CFI = .969, TLI = .962, RMSEA (90% CI) = .080 (.067-.094). The final model of the PRS consisted of 13 items.
EXTERNAL VALIDITY OF THE PRS
Correlations with the empathy and attachment dimensions were calculated in order to confirm the external validity of the PRS. To check the convergent validity, correlations between parental responsiveness and empathic concern and perspective-taking were calculated. To test the discriminant validity, correlations between parental responsiveness and personal distress and avoidance and anxiety in close relationships were calculated. Means, standard deviations, and correlation coefficients between the examined variables are presented in Table 3.
Table 3
Correlations between measured variables and the Parental Responsiveness Scale
Parental responsiveness was positively correlated with the two other-oriented aspects of empathy – empathic concern and perspective-taking – and was negatively correlated with avoidance in close relationships.
Mothers displayed higher levels of responsiveness (M = 82.15, SD = 9.46) than fathers (M = 79.27, SD = 8.04, t(248) = 2.18, p < .05, Z = –3.39, p < .001). However, there were no correlations between the parent’s age and their responsiveness towards their child. Moreover, parental responsiveness towards daughters (n = 127) was not significantly different to parental responsiveness towards sons.
DISCUSSION
This study confirmed the one-dimensional structure, reliability, and validity of the Parental Responsiveness Scale. Some modifications were made to improve this tool. Two items were removed to obtain better model fit indices. The scale measures parental sensitive responsiveness to their children’s cues. The PRS could be a useful tool for measuring the engagement of parents’ interactions with their newborn children from the first month of life to 18 months. The presented scale might facilitate the measuring of child-parent interactions and be useful for the subjective assessment of reactions in studies on predictors of parental responsiveness. Additionally, this tool could be useful not only as a subjective measurement of parental sensitive responsiveness, but also as an additional indicator alongside the objective scales typically implemented during naturalistic or laboratory observations of parent-child interactions. This would allow a relationship to be established between objectively measured sensitive responsiveness and the subjective perception thereof (Fekete et al., 2017).
As was hypothesized, parental responsiveness was linked to greater empathic concern and perspective-taking. As has been previously suggested, these two dimensions of other-oriented empathy are connected with focusing on others (Davis, 2004), displaying sensitivity to others’ emotions, and the ability to see things from another’s point of view. We might conclude that parental responsiveness as measured by the PRS scale requires effective emotional regulation, even when the experienced arousal is high and the situation is difficult to deal with (Eisenberg & Eggum, 2009).
However, hypothesis two was only confirmed partially, because parental responsiveness measured with the PRS scale was not related to lower levels of personal distress. This type of empathy is connected with self-focus and concentration on personal experiences while taking on the negative emotions of others (Schreiter et al., 2013). The lack of a significant correlation between personal distress and PRS suggests that even when parents are focused on their own emotions, they still respond to their child’s needs. Previous studies on mothers of children younger than 9 months reported that personal distress did not significantly affect the time they spent with their children on enriching activities (Jia et al., 2016). It is worth mentioning that greater levels of personal distress in social situations have been linked to greater attachment anxiety, stress, and greater difficulty maintaining satisfactory relationships (Davis, 2004). Therefore, such psychological factors may not be relevant in the relationship with one’s own child, as such relationships may differ in many aspects from other relationships.
The obtained correlations between PRS and parental attachment styles partially confirmed the third hypothesis. Only avoidance was negatively correlated with PRS results. Avoidance is related to negative patterns of attachment, which can influence interactions with the child and can impart negative emotions. It can make it more difficult for a parent to perceive a child’s cues and react to them promptly and adequately (van Ijzendoorn & Hubbard, 2000). Moreover, affective interpretation is decreased in individuals with avoidant attachment (Vriticka & Vuilleumier, 2012).
Anxiety in close relationships was not correlated with parental responsiveness, thus failing to confirm hypothesis 3. This lack of significant effect might have been caused by attachment anxiety being, on one hand, linked to experiences of more negative emotions in relationships and, on the other, with greater attentiveness to distress in others, including one’s own child. Anxious attachment is related to faster processing of all attachment-related information (e.g., a child’s cry), while, in avoidant attachment, processing is suppressed when negative cues occur (Vriticka & Vuilleumier, 2012). Consequently, anxious parents might not be less responsive to their child’s cues.
The differences in responsiveness between mothers and fathers can be explained through a sociocultural lens. Mothers participating in the study might be immersed in the Polish mother stereotype, and it has been confirmed that Polish women identify more with the role of mother than Polish men identify with the role of father (Kaźmierczak & Karasiewicz, 2019). On the PRS, mothers appeared to be more responsive than fathers, but this could just reflect their desire to present themselves as well as possible in their new role. Such an interpretation should be confirmed in observational and more objective studies.
LIMITATIONS
Despite the high reliability indicators and the clear construction of the presented scale, some limitations should be highlighted. The sample mostly consisted of mothers and parents who were well educated. Further research should focus on the application of the scale in more diverse samples. It should be emphasized that this scale has all the limitations typical of self-report measures. However, it is short and easy to implement when other research designs are not possible. Furthermore, it will be interesting to conduct further longitudinal studies using the PRS to measure the outcomes of parental sensitive responsiveness.
CONCLUSIONS
The Parental Responsiveness Scale is valid and reliable. It can be used in developmental psychology and psychopathology as a subjectively perceived and reported parental predisposition to react to a baby’s cues. It may be useful in both correlational and experimental studies (comparisons with observational scales; e.g., the Ainsworth Sensitivity Scale) that focus on individual differences between parents or temperamental and dispositional predictors of the measured construct. Moreover, in applied psychology, it may be beneficial to identify parents who have difficulties perceiving, understanding, and/or reacting adequately and promptly to their child’s cues (e.g., because of depression).